Sport, exercise and osteoporosis
Authors: Eva Heinen, graduate sports scientist (Univ), Prof. Dr. med. Edgar Heinen
Osteoporosis is a systemic skeletal disease characterized by a decrease in bone mass (bone density) and a less stable microarchitecture of the bone tissue. This increases bone fragility and susceptibility to fractures. If fractures have already occurred as a result of osteoporosis, we speak of manifest osteoporosis.
The human skeleton consists of 220 bones with different structures: In addition to the long bones, there are spongy bones, e.g. in the vertebral bodies, which are constructed like a sponge surrounded by a solid shell (corticalis). The individual bone beams (trabeculae) are arranged like the struts of a building crane in such a way that they ensure optimized pressure and tensile strength for the required requirements.
A particularly good example of this trajectorial structure is the femoral neck, which can be compared to a reinforced concrete structure used in modern construction. It consists of tension-resistant connective tissue fibers – the steel framework – and pressure-resistant lime salts, which correspond to the concrete component. The mixture of the two gives the bone both strength and elasticity, which ensures a high load-bearing capacity.
Many years ago, it was shown that the organism is able to adapt this trajectorial structure of the bone to changing loads by building up and breaking down. The control of the remodeling seems to come from the finest extensions of the bone cells (osteocytes), with which the load is constantly measured and the remodeling is determined. All in all, the malleolar bone is “remodeled” in about three years, the long bone in about five years, together with the necessary adaptations.
Bone density measurement
An important factor in assessing bone strength is bone density, which is usually measured using dual photon absorptiometry. Unfortunately, device manufacturers have not yet been able to agree on a standard. Therefore, the results obtained differ depending on the device used. A situation that is actually unacceptable for a physical measurement method. Instead of a clearly defined value for bone density (in g/cm²), you have to deal with the T-score and the Z-score if you want to compare the results measured on different devices. Absurd: the measurement to check whether a measure has had any effect should always be carried out on the same device as the initial measurement!
A T-score of – 1 means that the bone density of the person examined is 1 standard deviation lower than that of healthy 30-year-old women or men measured on a device from the same manufacturer. If the measured T-score is below – 2.5, the person examined has osteoporosis by definition (WHO). To make the whole thing even more opaque, the Z-score has also been defined. For negative values, this indicates how many standard deviations lower the value is than for women or men of the same age. As bone density typically decreases with age, this value is therefore higher than the T-score. (P.s. -1.0 is > than – 2.5!) The background to the definition of the Z-score is the consideration of whether people with a bone density similar to that of the age group should be treated at all.
In osteology, it is rightly assumed that the highest possible individual peak bone mass offers a certain degree of protection against osteoporosis-related bone fractures. More physical activity, especially muscle training in youth and early adulthood, is therefore a protective factor against the development of osteoporosis. But even in old age and during the menopause, higher muscle mass is likely to be associated with higher bone density. However, it must be assumed that muscle mass can be stimulated much more quickly (weeks to months) than bone, which needs at least many months before it increases significantly in mass as a result of greater stress.
Connection between muscles and bone mass
Our organism is obviously constructed in such a way that it reduces systems that it only needs a little. If you lie in bed for many weeks, the size of your heart, your stroke volume, your muscle mass and even your bone mass will decrease and atrophy. The body adapts its tools to its needs. Conversely, more exercise leads to an increase in stroke volume and the size of the heart, to an increase in muscle mass and strength. Even bone growth is stimulated in the areas that are particularly stressed – a “breathing system”.
Dual-photon absorptiometry can be used to determine the bone mineral mass of the entire body in addition to the bone density of the vertebral bodies and femoral neck. This value is understandably highly dependent on body size. By dividing the bone mineral mass by the body height² (analogous to the BMI), the bone mineral mass index can be calculated, which – like the BMI – is independent of body height. Dual-photon absortiometry can also be used to determine the muscle mass index (MMI), which is independent of body size.(see Dexa method).
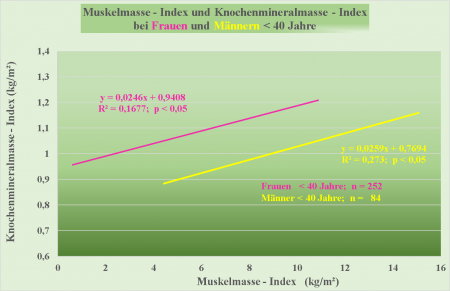
There is a significant correlation between the muscle mass index and the bone mineral mass index for both women – pink line – and men – yellow line. Only the 252 out of 709 women and only the 84 out of 297 men who were younger than 40 in Eva Heinen’s thesis were examined. The women all still had a regular menstrual cycle.
If all subjects over the age of 40 were included in the study, the correlation was no longer significant. This is probably due to the increasing osteoporosis with age on the one hand and the increasing appositional bone growth as a result of osteoarthritis and increasing calcifications on the other.
Of particular interest to endocrinologists is the fact that the mean value of the bone mineral mass index was measured almost identically in men and women at 1.01 and 1.03 kg/m² respectively. However, the correlation showed practically a parallel shift in the trend curves: women consistently had a 0.17 kg/m² higher bone mineral mass index than men with the same muscle mass. We are currently working on a publication to explain this phenomenon.
Musculature and osteoporosis-related fractures
In addition to muscle mass as a stimulus for bone growth, other muscular factors play an important role in preventing fractures. Muscle strength per se can prevent or mitigate a fall or two; good muscle coordination based on regular exercise is crucial for preventing falls, the main cause of bone fractures. (see illustration below).

The next figure shows the relationship between the force applied and the probability of a fracture as a function of bone density.
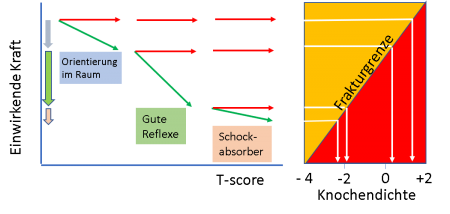
On the right-hand side of the illustration, the principles of materials science are applied to the conditions on the bone. If the force applied is greater than the fracture threshold (for the bone: the fracture limit), the bone will break. It can be assumed that the lower the T-score, the sooner the bone will fracture (cave – 4 < – 2!). This part of the illustration should show that any bone – regardless of stability (bone density) – can break if the force applied is high enough!
The top row of red lines on the left shows what was regularly seen as a medical assistant during his time as a surgeon near Düsseldorf’s old town: An excess of alcohol had repeatedly put mostly men in a state where they had lost their orientation in the room, tipped backwards with their chair and hit the back of their head without any reflexes. As there is hardly any fat mass on the back of the head that could have served as a shock absorber, skull fractures were not that rare.
Orientation in space and, in particular, good reflexes would probably have prevented the fall, or at least cushioned it, as the typical reflex in such a situation is to pull the head in and put it down on the chest, thus considerably reducing the force acting on the back of the head.
By far the greatest contribution to reducing the force applied is therefore made by reflexes, which are the result of the performance of the nervous system and the muscles. The greater the strength of the muscles, the more likely it is that a fall can be avoided or mitigated.
It is astonishing that, despite the overwhelming number of studies, the DVO (German Osteology Association) guidelines for the prevention of osteoporosis through sport and musculature and for supporting therapy, or better still, as an important pillar of therapy, only state: “Regular physical activity should be encouraged with the aim of improving muscle strength, balance and coordination. Immobilization should be avoided.” The information provided by the German Osteoporosis Self-Help Association is much more useful in this respect: in their brochure, exercise is mentioned with many well-documented statements before the description of drug therapy, which is often unavoidable.
So here are a few tips.
Endurance training (walking, cycling, swimming) has many positive effects on almost all bodily functions. However, many studies have shown that endurance training alone cannot stimulate bone growth. Most experts therefore recommend strength training to reduce the risk of osteoporosis(you can find a good overview article here). However, if there is already a considerable reduction in the calcium salt content of the bone, this must be taken into account in the form of lower loads (weights). Excessive weights, especially with the upper body bent forward, should be avoided.
In a study by Uusi-Rasi et al. 2015 from Finland It was shown that even in 70 – 80 year old women with moderate strength training 2 x / week and additional exercises 5 – 15 minutes per day, a significant increase in muscle strength can be achieved and that the group that performed the strength exercises only suffered half as many fractures as the comparison group. So: even with increasing age, you can clearly train your muscles and thus maintain your quality of life!
However, overloading must also be urgently advised against, especially at the beginning of strength training. Today, it must be assumed that there are sensors (extensions of osteocytes) in the bone that measure the force applied. If a significantly higher load is measured, so-called osteoclasts (bone-degrading cells) are activated first. Initially, there is even increased bone resorption. Only then do the osteoclasts trigger the osteoblasts, which increase the bone substance. (bone remodeling unit).
In the case of new bone construction, everything is similar to the expansion of a highway. Initially, increased traffic volumes are reported. The unavoidable construction site to upgrade the highway inevitably results in more traffic jams at the beginning. Only after the expansion can more traffic be handled. However, the good thing is that a cycle of the “bone remodeling unit” takes about 3 months in total, not as long as some roadworks on the freeway!