Spiroergometry
Spiroergometry is a procedure in which the reactions of the heart, circulation, respiration and metabolism – indirect calorimetry – can be examined and quantified by measuring the volume and concentration of respiratory gases during defined physical exertion. If you leave out the work, you can simply measure the basal metabolic rate with spirometry and additional determination of the respiratory gases – one reason why endocrinologists have been working with this method for a long time.
In detail, the following parameters are continuously recorded during the investigation:
- Heart rate (beats/min)
- RR syst and diast. (mm Hg)
- Respiratory rate (breaths/min)
- Tidal volume (ml / breath)
- Respiratory minute volume (ml / min)
- Oxygen uptake; VO2 (ml O2 / min)
- CO2 output; VCO2 (mlCO2 / min)
- Respiratory exchange rate (RER)
mlCO2 / min / ml O2 / min - end-expiratory O2; Pet O2 (mm Hg)
- end-expiratoryCO2 pressure; PetCO2 (mm Hg)
Other parameters can also be determined. We are interested in the following:
- VO2max: maximum oxygen consumption (ml / kg body weight); corresponds to maximum performance.
- VT1 (ventilatory threshold 1): The exhalation ofCO2 increases more than the intake of O2, the RER increases. Corresponds approximately to LT1 (the lactate threshold1)
- VT2 (ventilatory threshold 2 = RC point) The increase in respiratory minute volume is greater than the increase inCO2 exhalation. (corresponds approximately to LT2 (the lactate threshold 2).
- the RQ, the respiratory quotient, which is calculated from the ratio of exhaledCO2 to absorbed O2 and provides information on how much of the energy used is produced from the oxidation of glucose or fatty acids.
- Why the RQ should more correctly be called RER(respiratory exchange rate), can be found here.
How does spiroergometry work?
The early beginnings of spiroergometry date back to the end of the 19th century. The older of the two authors used the Douglas bag, a very large balloon with which gas exchange was measured, to carry out his first basal metabolic rate tests. Errors in handling and calculation were easy to make!
Today, the test person puts on a tight-fitting plastic mask that is connected to measuring sensors. The sensors are extremely small and the data is recorded on a device the size of a cell phone! This means that today’s spiroergometers can even be used outdoors without any problems.

If you have calibrated correctly, if there is no leak, if the air seal is complete with the outlet held shut at the end of the mask, then achieving reproducible results on the ergometer, even outdoors, is no longer an art. However, the interpretation of the measurement results, especially for the various medical issues, requires specific experience for each of the subjects!
In general, spiroergometry distinguishes between two different exercise regimes:
- the ramp load, in which the load is increased in small steps, usually every 30 seconds,
- the step load, in which a defined increase should be made every 3 – 4 minutes in order to achieve an approximate steady state of the lactate.
If a test subject is being tested for diseases, an ECG should always be included. Well-defined, clear exclusion and termination criteria apply to spiroergometry.
What is the purpose of spiroergometry?
As spiroergometry provides information about many of our body’s functions, it is used in many medical disciplines and in sports science to answer exciting questions.
- Assessment of cardiopulmonary performance
- Clarification of heart disease
- Question of exercise-induced hypertension
- Gas exchange disorders in the lungs
- Preoperative performance check
- Expert performance analysis
- Metabolic tests at rest and under stress
- Training control for athletes
- Training control for sports enthusiasts
The various medical indications and interpretations will not be discussed in this article. There are plenty of publications and textbooks on this, as well as more competent authors than us!
On our homepage, however, we would like to deal with the aspects of spiroergometry in metabolic examinations and for training control in sport.
Indirect calorimetry
According to Wikipedia, a calorimeter (lat. calor:heat’; metari, to measure) is a Measuring devicefor determination the amount of heat that is released or absorbed during physical, chemical or biological processes. In other words, you measure how much heat, for example, a person produces in an enclosed, very elaborately shielded room.
With the indirect calorimetry the calorie consumption is calculated indirectly via the measured oxygen consumption. In humans and animals, it can be assumed that an average of 4.85 kcal is released per liter of oxygen. However, it makes a difference how much fat (4.68 kcal/l O2 ), protein (4.8 kcal/l O2 ) or carbohydrate (5.05 kcal/l O2) is used for energy production at the time of measurement; the caloric equivalent is therefore dependent on the RER, the ratio of exhaledCO2 / absorbed O2and can be calculated with greater accuracy using the following formula:
- Cal. equivalent = (1.233 * RER + 3.85) kcal / l O2
For those who have already switched to joules: - Cal equivalent = (5.14 ∗ RER + 16) kJ / l O2.
Respiratory quotient (RQ) or respiratory exchange rate(RER)
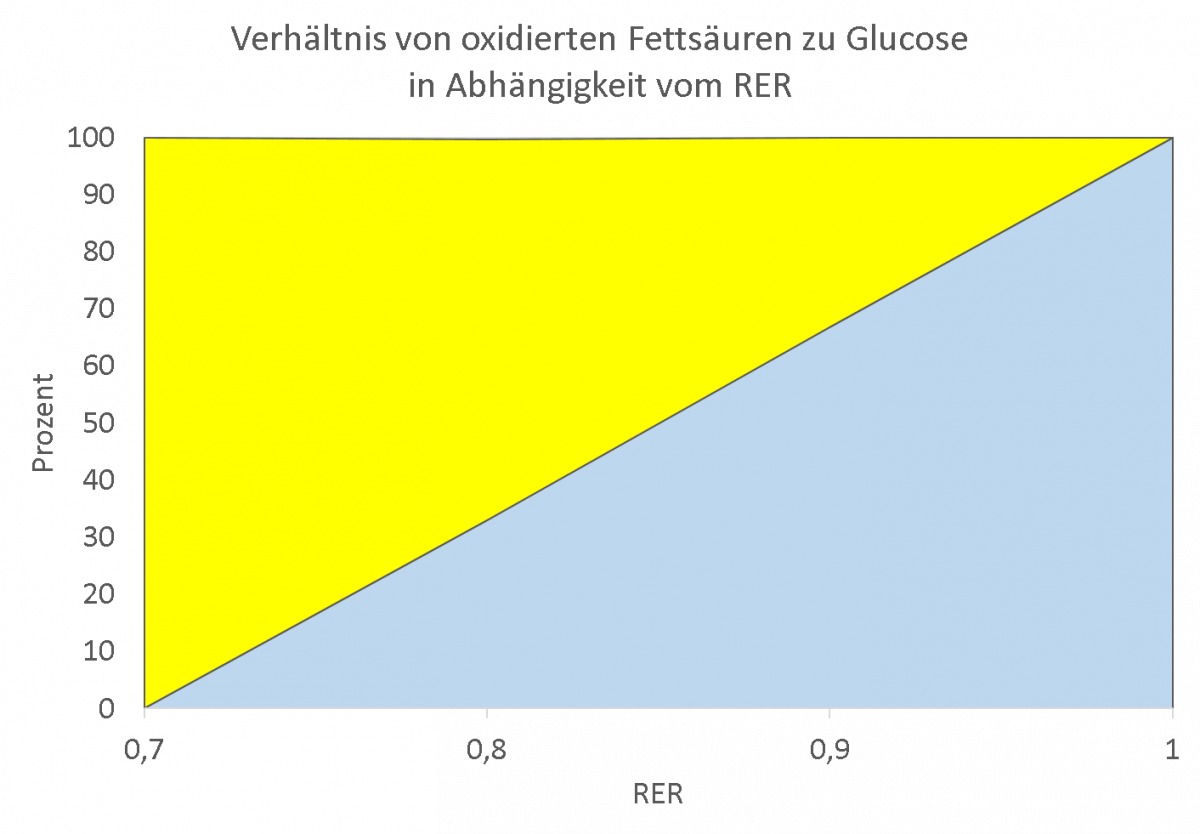
From the ratio of exhaledCO2 to absorbed O2, it is possible to deduce (without taking into account the oxidation of proteins) how high the proportion of glucose or fatty acids is in energy production.
Why?
The oxidation of glucose requires 1 mole of O2 for every 1 mole ofCO2, whereas the oxidation of fatty acids only releases 0.7 moles ofCO2 per mole of O2.
Glucose oxidation: C6H12O6 + 6 O2 → 6 CO2 + 6 H2O + 36 ATP
CO2 produced / O2 consumed = 1 (respiratory quotient)
Fat oxidation: C15H31COOH + 23 O2 → 16 CO2 + 16 H2O + 129 ATP
CO2 produced / O2 consumed = 16/23 = 0.7 (respiratory quotient)
The respiratory quotient can be used to calculate the percentage of glucose or fatty acids in the energy supply.
However, as shown in the chapter on the fat burning pulse and under RER and hyperventilation, the RER can only be used to draw conclusions about the proportion of glucose and fatty acids in energy production if there are no other sources for the amount of exhaledCO2; a fact that the main protagonists of spiroergometry already reported in the 1960s, but without quantifying the proportion that e.g. buffering of lactate through increased exhalation of CO2 via the lungs has.However, they did not quantify the role played by the buffering of lactate through increased exhalation ofCO2 via the lungs, which we have made up for in the chapter“Fat-burning pulse“.