Hyperventilation and RER
The respiratory exchange rate (RER) of VCO2 to VO2 can only be used as a measure of the proportion of glucose or fatty acids in the energy supply if there is no other source of exhaledCO2 than the product of the oxidation (CO2) of substrates.
How massively increased breathing, hyperventilation, can influence the RER is shown by the self-experiment depicted in the figure.
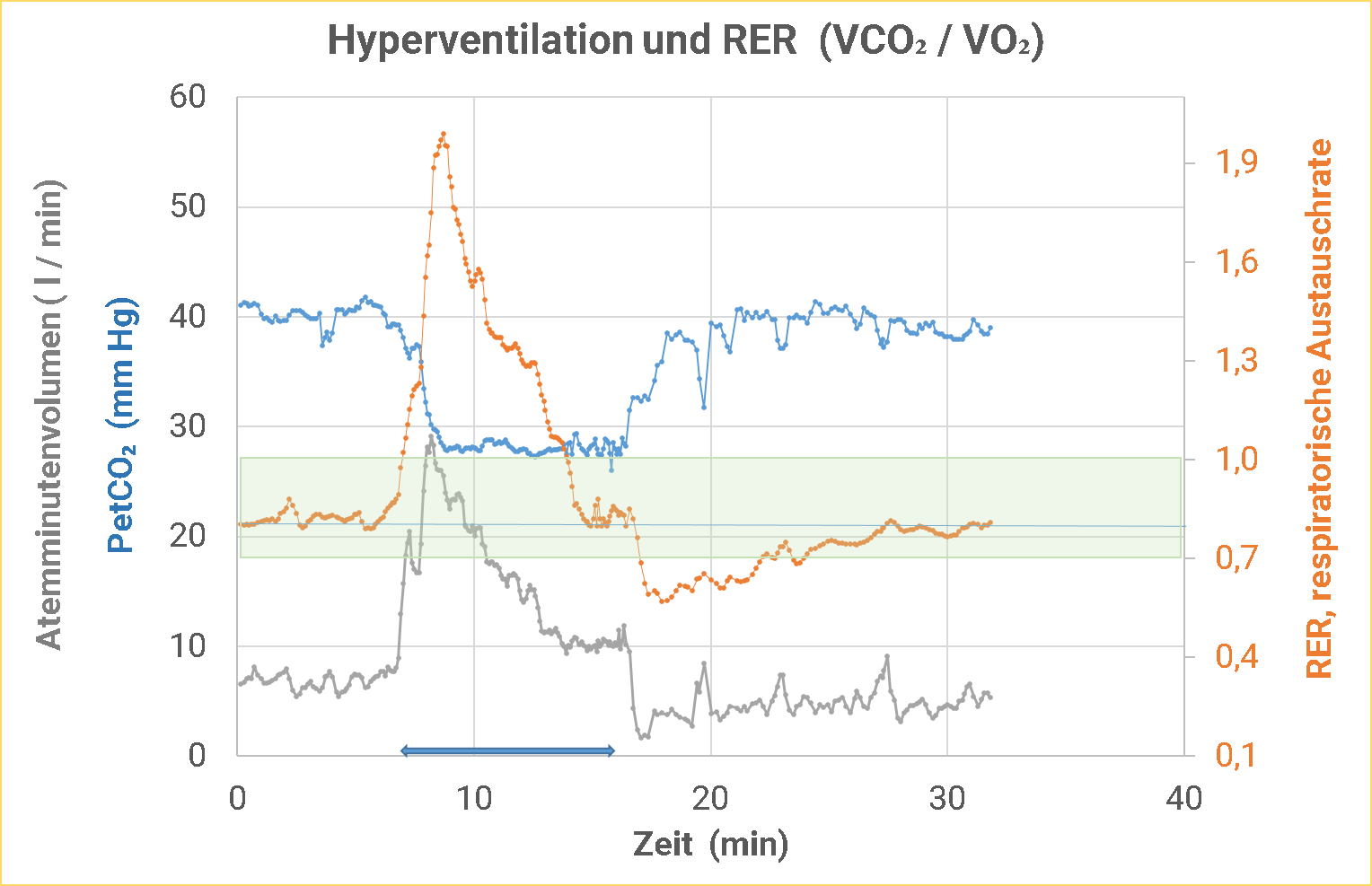
In the self-experiment shown above, hyperventilation is demonstrated by the PetCO2 reached, thepartial pressure of CO2 at the end of the exhalation phase. Under normal conditions, this is between 35 and 45 mm Hg. At the beginning of the experiment, the PetCO2 was just above 40 mm Hg. The respiratory minute volume at 7.5 l. Under these “resting” conditions, a RER of around 0.8 was measured.
After 7 minutes, the respiratory minute volume was rapidly increased until a PetCO2 of < 30 mm Hg was reached. For the subject’s orientation, the PetCO2 was constantly visualized on the spirometer. After the initially necessary massive hyperventilation to achieve a low PetCO2, the respiratory minute volume could be successively reduced while maintaining the PetCO2 below 30 mm Hg. After about 7 minutes, a steady state was reached with a respiratory minute volume of just over 10 l.
The RER increased to values up to 2 within a very short time with the onset of hyperventilation! Biochemically, there is no metabolic process in which such a result could occur as a consequence of energy provision! Values just above 1 can be reached at most with the stuffing goose, if it makes fats out of the massively added carbohydrates! The additional exhalation ofCO2 triggered by hyperventilation completely falsifies the RER! From various spiroergometry equipment manufacturers, the ratio of glucose to fatty acids used to provide energy is calculated for each breath. A short, deep breath by the test person significantly increases the exhalation ofCO2 and significantly reduces the intake of O2. The RER rises immediately. This has nothing to do with a different ratio in the provision of energy at the cellular level. The procedure to indicate from breath to breath significantly changing ratios of fats to glucose in the energy supply is completely absurd and should absolutely be removed from the software!
However, in the further course of hyperventilation, the RER decreased again and reached the initial value again after about 7 minutes in the steady state of hyperventilation! From this point on, no additionalCO2 was released into the breathing air due to hyperventilation! During this time period, the RER should again represent an indication of the glucose to fat ratio in energy provision.
After a total of 10 minutes, the hyperventilation was quickly terminated by conscious hypoventilation, which can be seen from the rising PetCO2 values and the very low respiratory minute volume. Normal PetCO2 values were reached again after about 6 – 7 minutes.
The RER dropped sharply to 0.57, a value that can only be explained by a retention ofCO2 in the organism. By the end of the experiment, the RER then increased back to baseline.
Quintessence:
- At the onset of hyperventilation, the RER increases massively.
- In the steady state, hyperventilation has no measurable effect on the RER, which then again allows a conclusion to be drawn about the ratio of glucose to fatty acids during energy provision.
- When hyperventilation subsides or ceases, the RER decreases substantially, even to values below metabolic possibilities.
- An interpretation of the VCO2/VO2 ratio for each breath does not make sense; a short sigh would be incorrectly interpreted as an increase in the ratio of glucose to fatty acids in energy production.
PS:
The subject did not feel well during hyperventilation: he had slight dizziness, tingling around the mouth, ice-cold hands: typical symptoms of hyperventilation. s also Eva’s film on you tube: Stress, stress hormones and hyperventilation.